Serving all the provincial residents within an Eastern Province
The client requested guidance on how to achieve their strategic goals that would address the quality, accessibility, and efficiency of the provincial healthcare system. The two main hurdles to overcome were how to improve patient, client and resident access to all services and to improve population health outcomes. The goal was to reduce the Overall Average Length of Stay (OALoS) by 50%. This required a focus on the extra time spent in the hospital above the expected stay length to address improving patient flow through Acute Care (hospitals). The first phase of the program was affectionately known as “reducing the hospitals’ reasons for poor patient flow”. Phase one was designed to identify the ‘External to Acute’ care reasons for excessive admissions and discharge delays. This would address blocked beds in emergencies; patients that had no assigned primary care providers; missed communications for sending patients home with home care; and hospital admissions from long-term care to name a few.
Our healthcare experts were engaged to design and guide a province-wide health system transformation using Lean Six Sigma and quality management implementation and training techniques. This included leadership training and consultation, as well as a training and mentorship program to create Yellow, Green, and Black Belt-level personnel that would manage quality improvement projects across the province. The focus on training health system staff was to build their internal quality improvement capacity, leading to long-term sustainability after the consulting engagement was completed.
The team developed a two-phase approach to reduce the OALoS in Acute Care.
Phase l:
The team focused on the areas external to the Acute Care system that could contribute to increased acute care patient flow, including Public Health, Primary Care, Home Care, Long-Term Care, and Extended Care. The following projects outline some of the changes initiated:
Phase ll:
Once these Acute Care external factors had been addressed, Phase II focused directly on solutions for the two primary hospitals. This included:
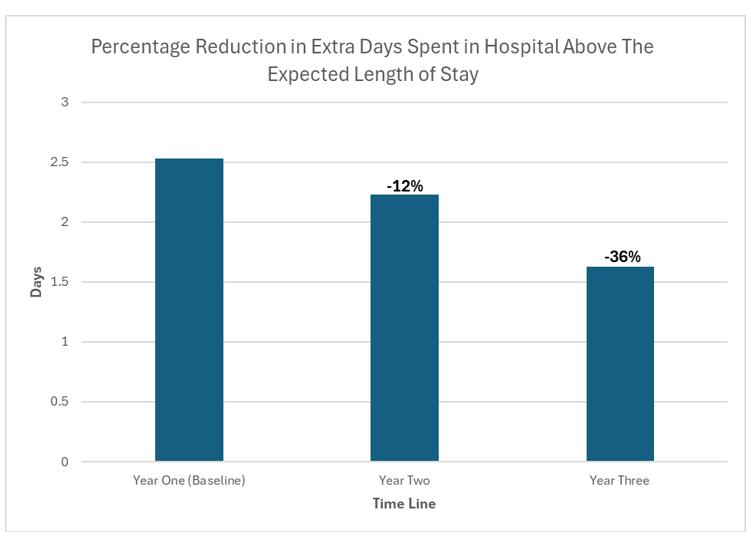
As a result of this Quality Management System transformation, our client was equipped with the foundation, trained staff, infrastructure, and systems to continue its quality improvement journey independently. Realized benefits through this engagement included: